Breeder/Exhibitor Ed, Health
Written by Dr. Alice Crook and taken from the Canine Inherited Disorders Database with permission
related terms: chronic liver disease, copper-associated hepatitis/copper toxicosis in Bedlington Terriers, chronic active hepatitis, Doberman hepatopathy, chronic inflammatory hepatic disease
What is chronic hepatitis?
Chronic hepatitis is a catch-all diagnosis for a number of diseases where there is inflammation and death of liver tissue. Affected dogs develop a slowly progressive liver disease. There are many possible causes including viruses, bacterial infection, and some drugs. A familial predisposition to the development of chronic hepatitis exists in some breeds, although the cause is unclear. These breeds are listed below.
In Bedlington Terriers and West Highland White Terriers, an inherited defect in the metabolism of copper is known to cause chronic hepatitis (copper-associated hepatitis/copper toxicosis in Bedlington terriers). It is estimated that 25% of Bedlington Terriers have the disorder, and 50% are carriers (i.e.. they will not become ill, but can transmit the disorder to their offspring). Copper accumulation occurs in some other breeds as well, but whether the excess in copper is the cause or the result of liver disease is unknown.
How is chronic hepatitis inherited?
Inheritance in the Bedlington Terrier is autosomal recessive. The mode of inheritance is unknown in other breeds.
What breeds are affected by chronic hepatitis?
Doberman Pinscher (predominantly female dogs affected), American and English Cocker Spaniel, Skye Terrier, Labrador Retriever.
Copper-associated hepatitis – Bedlington Terrier and West Highland White Terrier
For many breeds and many disorders, the studies to determine the mode of inheritance or the frequency in the breed have not been carried out, or are inconclusive. We have listed breeds for which there is a consensus among those investigating in this field and among veterinary practitioners, that the condition is significant in this breed.
What does chronic hepatitis mean to your dog & you?
The liver has a large reserve capacity, meaning there must be damage to a significant portion before you will see any signs of illness in your dog. The first signs of liver disease are generally vague and non-specific, and include loss of appetite, vomiting, weight loss, depression, lethargy, and/or increased drinking and urination. As the disease becomes advanced, there will be signs more specific to liver failure such as jaundice (you may see yellowing of your dog’s eyes for example), coagulation problems, fluid accumulation (ascites), extreme weight loss, and neurologic abnormalities (hepatic encephalopathy) such as head pressing or behavioral changes, due to the build-up of toxins normally metabolized by the liver.
In affected Bedlington Terriers, there is progressive accumulation of copper in the liver over time. Associated liver disease may manifest itself in 3 ways.
1) Young dogs (less than 6 years of age) may suddenly develop signs of liver failure, including vomiting, depression and lethargy. Most will die within a few days despite intensive therapy. Others will recover over a few weeks, and thereafter experience occasional milder bouts that may be associated with stressful events such as showing or traveling.
2) In middle-aged to older dogs, similar but less severe signs develop insidiously and the disease has a more chronic course. Gradual weight loss and deterioration in condition are common initially, while specific signs of liver disease (as listed above) develop in the advanced stages of the disease.
3) Young as yet clinically unaffected dogs may be found to have elevated liver copper and biochemical/pathological changes associated with liver disease. These are the dogs in whom treatment will be most effective.
West Highland white terriers are also affected by a disorder of copper accumulation, but the magnitude of increase is less. Diagnosis, signs of illness, and principles of treatment are similar to the Bedlington Terrier.
How is chronic hepatitis diagnosed?
Before liver disease reaches an advanced stage, the clinical signs are generally vague and non-specific. Your veterinarian will do some routine diagnostic blood tests which will show elevations in liver enzymes. This is investigated further with specific liver function tests. Once the problem has been pin-pointed to the liver, your veterinarian will take a liver biopsy which will be sent to a veterinary pathologist. This is necessary to differentiate chronic hepatitis from other causes of liver disease (such as liver cancer or an infection), and to determine the severity and extent of the problem.
For the veterinarian: Elevated ALT is the most consistent biochemical abnormality. With acute onset hepatic necrosis there may be hepatomegaly. With chronic advanced disease, the liver is small and not palpable due to fibrosis and cirrhosis.
Liver biopsy is required for definitive diagnosis of chronic hepatitis, to characterize the extent of fibrosis and progression to cirrhosis (which is by definition irreversible and indicative of a poor long-term prognosis), and also to quantify hepatic copper levels. The key histopathologic feature is moderate to severe inflammation. The role of hepatic copper accumulation is controversial. Copper is commonly elevated, but this is believed by most to be secondary to the chronic inflammation, in contrast to the primary copper accumulation that causes copper-associated hepatitis in Bedlington and West Highland white terriers.
Copper-associated hepatitis should be suspected in any Bedlington terrier with physical or biochemical evidence of liver disease, and biochemical screening should be done in any Bedlington terrier with a vague illness. Asymptomatic affected dogs can be detected through biochemical screening (2/3 will have elevated ALT), liver biopsy, or a radioisotope study using copper-64. Affected dogs will have reduced stool radioactivity compared with normal dogs, due to reduced biliary excretion of copper. A genetic marker has been identified for copper toxicosis in Bedlington Terriers that will detect affected and carrier dogs at any age – see www.vetgen.com
How is chronic hepatitis treated?
Unfortunately, liver damage is often advanced by the time the disease is recognized. Depending on the stage of your dog’s illness when it is diagnosed, treatment may involve intravenous fluids, antibiotics, corticosteroids, dietary management, and possibly medication to reduce copper levels in the liver. Your veterinarian will discuss with you the prognosis for your dog.
In Bedlington Terriers, there are a few different drugs to control copper accumulation in the liver. These must be given for the life of the dog to prevent further build-up of copper. If the disorder is detected early, when there are no or few clinical signs, these drugs will allow many dogs to live out a normal life.
For the veterinarian: In Bedlington Terriers, D-penicillamine (copper chelator which promotes urinary copper excretion), trientine hydrochloride (an alternative copper chelator) or zinc therapy (decreases intestinal copper absorption) may be used to gradually reduce hepatic copper content and prevent further accumulation. Treatment is similar in the West Highland White Terrier. Because copper accumulation is not continuous throughout life in the Westie, mature dogs may not require chelation therapy, depending upon hepatic copper levels.
Unfortunately, hepatic liver damage is generally advanced by the time a liver biopsy is taken and the disease is recognized, leading to a poor prognosis. Improvement may occur with prednisone therapy. The usefulness of copper chelation therapy in breeds other than the Bedlington and West Highland White Terrier remains unclear.
Breeding advice
A genetic marker has been identified for copper toxicosis in Bedlington Terriers that will detect affected and carrier dogs at any age – (see www.vetgen.com) Because of the prevalence of this serious disorder in the Bedlington Terrier, all dogs to be used for breeding should be tested. The results may be registered with the Orthopedic Foundation for Animals (see www.offa.org) Testing may also be done by liver biopsy but dogs must be older than 1 year of age so that sufficient copper accumulation will have occurred to be detectable.
There is no similar testing available for other breeds. Affected dogs should not be bred, and breeding of their parents should be avoided as well.
FOR MORE INFORMATION ABOUT THIS DISORDER, PLEASE SEE YOUR VETERINARIAN.
Resources
Johnson, SE.1995. Diseases of the liver. In S.J. Ettinger and E.C. Feldman (eds.) Textbook of Veterinary Internal Medicine, pp. 1313-1357. W.B. Saunders Co., Toronto.
Leveille-Webster, C.R. and Center, S.A. 1995. Chronic hepatitis: therapeutic considerations. In J.D. Bonaguara and R.W. Kirk (eds.) Kirk’s Current Veterinary Therapy XII Small Animal Practice. pp. 749-756. W.B. Saunders Co., Toronto.
Twedt, D.C. 1997. Treatment of chronic hepatitis. ACVIM- Proceedings of the 15th Annual Vet. Med. Forum, pp.234-236.
Leveille-Webster, C.R. 1996. Medical management of inflammatory hepatic disease in dogs. ACVIM-Proceedings of the 14th Annual Vet. Med. Forum, pp. 43-44.
Orthopedic Foundation for Animals, Registry for Copper Toxicosis in Bedlington Terriers, www.offa.org
Breeder/Exhibitor Ed, Health
by Mervi Ihantola DVM
Introduction
|
Chronic active hepatitis (CAH) is a yet relatively unknown liver disease with dramatical consequences for the Dobermann. The disease was first discovered by us in Finland at the end of the 70s. Articles in medical journals began appearing in the beginning of the 80s in the USA. As there is too much copper in the liver, the condition has been also called copper toxicosis. Other names used for CAH are chronic hepatitis and Dobermann hepatitis. The symptoms are so typical of CAH patients that they caught the eyes of the Finnish Dobermann breeders in the 80s. This led to the beginning of an eradication program. This disease is recognized worldwide as data has been published at least in USA, Finland, Holland, Sweden, Germany, England, Australia. |
Signs
|
The disease is most likely to affect a female aged four to six years. Males seldom develop CAH. The initial symptom, though often neglected, is polydipsia (heavy drinking). The dog may eat a lot of snow during the winter and tends to seek some other sources of water, besides its own cup. Heavy drinking may only be temporary or intermittent. When the condition progresses further, a poor appetite vomiting and weight loss soon follow. As the disease advances, the mucous membranes start to turn yellowish. This is most apparent in the eyeballs (sclera), the gums and on the skin in areas where hair is scarce such as the ears and the inguinal region. This stage is called icterus and is typical of any liver condition because bilirubins (bile pigments) accumulate in the blood stream and tissues due to the liver dysfunction. Weight loss becomes accelerated and the dog develops free fluids in the abdomen, often so much that it looks like a puppy that has just eaten a huge dinner. The only differences in the appearance are the pronounced ribs and spine. The dog is tired and lethargic, although not entirely incapable of running and playing if required, as Dobermanns always like to do. |
History
|
The Finnish Kennel Club supported the start of a wide based collection of blood samples from healthy Dobermann females in 1987. We anticipated to find changes in liver enzymes like ALT (s-ALT) from normal dogs before the onset of clinical signs. The suspicions proved to be valid. The serum ALT values were clearly elevated for a long time before the individual itself showed any signs of the disease. As a matter of fact, as the project has continued we have noticed that some dogs with elevated liver enzyme values may develop the clinical signs quite late. Only the elevated liver enzymes indicate the presence of problems in the function of the liver. The right nutrition among other yet unknown reasons is believed to play an important role in keeping the individual from developing symptoms. This is not surprising considering the responsibility the liver takes in metabolism; it becomes over loaded with the wrong nutrition. |
Eradication program
|
In Finland, we want to discover the sick animals long before the problems show up. During the years we have collected blood samples from dogs that do not present any signs of the disease. A majority of the test are normal of course continuously. The ideal procedure is to start investigations at the age of two to three years and continue yearly or every two years up to the age of about seven years. Nowadays CAH testings are official and obligatory for Dobermanns which are used for breeding. To get puppies registered, both parents must have results no more than ten months old at the time of the mating.
Every now and then we discover individuals with abnormal values. Many of them are just innocent, once in a life time jumps, but few of those elevated values remain high. These are the dogs that should be to followed by blood tests. The definitive diagnosis of CAH is made only by biopsies taken from the liver. That is recommended for individuals with high ALT values for two to three consecutive tests or several high peaks during one year. We are able to detect any deterioration at their health condition by following the test values. Those Dobermanns with ALT values over the normal laboratory range (VETLAB, Tampere; the normal range is 24 – 136 U/I ) more than once, are also controlled for SAP, bilirubin, bile acids, and if needed, other blood parameters to get more information about the situation and to know more about the prognosis. Different laboratories have different normal ranges for ALT. In order to obtain reliable and comparable results, qualified lab is needed. In Finland, we approve only one lab for official tests by Finnish Dobermann Club / Finnish Kennel Club.
|
Treatment
|
What if the dog gets the clinical signs? Then the situation is worse. Blood tests may show s-ALT to be five to ten times over the normal. Other blood parameters are often not good either. At the moment we do not know the cause of the disease and it is very difficult to try to cure CAH with specific treatment. We have to try the medicines which relieve the symptoms. Initially, drugs which chelated the copper (D-penicillamine) were used. This didn’t seem very encouraging. It would seem that copper is not the reason for the liver damage, as is the case in Bedlington hepatitis. Copper appears only secondary and not in the excessive amounts of Bedlington. The most valuable medicine is still corticosteroids. On the other hand, steroids and the Dobermann is not a good combination and the use of this medicine can result in some problems. It seems that the breed is sensitive to its use. Corticosteroids often results in side effects which we would prefer to avoid. The treatment of clinically ill dogs demands a lot of precision and caution. With the proper treatment, it is possible to ease the progress of CAH and prolong the inevitable a little further. The difference between the beginning of the symptoms and the start of the treatment makes a great difference in survival time. According to our statistics, the survival time can be from some weeks to several years. New medicines to treat patients with CAH are continuously being researched, but until this day we do not have many promising alternatives. We prefer a strict diet based on home-made food low in copper and abandoning all commercial preparations. The food regiment is the same for dogs with no clinical symptoms. |
Discussion
|
Just by controlling all breeding stock, the number of CAH cases seems to be decreasing. We had great difficulties in the 80s just before our quarantine system for dogs was abandoned. Most individuals were related to some heavy used carriers of CAH. In 1988 and onwards we were able to import many new Dobermann lines. It seemed to help a lot. Or perhaps the problem is just hidden by some of the owners and breeders? Anyway it is almost impossible to breed with individuals with high ALT results nowadays in Finland. Not because it is not allowed (because it is, only test has to be made), but mostly because the results are public. Public opinion is important in selling the puppies. We are not free from CAH. Our first recognized cases to Finland came with the
imported animals from Germany. We have still found many individuals with CAH to have direct ancestors of imports or are imported themselves. So it is not possible to stand against CAH alone. It is sad that we are dependent on European breeding stock, which is totally out of control with CAH. That is of course mainly because breeders and veterinarians are not aware of the problem called CAH. The problem can come more common again in Finland, but also elsewhere due to two reasons. We sometime use some males heavily all over Europe not knowing their health state and population number can drop quickly in the near future because of the ear and tail cropping legislations, leading to serious genetic problems . |
Breeder/Exhibitor Ed, Health
*It is perfectly normal for young dogs to lose their deciduous, or “baby,” teeth much as human children do. Canines have 28 deciduous teeth and 42 permanent teeth.
The small teeth in the front of a dog’s mouth are the incisors; there are six on the top and six on the bottom. Canines, the sharp “fanglike” teeth, total four; two on top (one to each side of the set of incisors) and two on the bottom. Located to the side of the canine teeth, the 12 deciduous premolars will be replaced by 16 permanent teeth. Molars are the teeth located farthest back in the mouth; they are part of the permanent set of teeth only and there are ten of them.
A dog´s health can suffer if their teeth or gums are giving them trouble. Dental exercise (raw beef bones, chew bars etc.), a balanced diet and teeth cleaning with a canine toothbrush and paste are helpful in keeping your dog´s teeth healthy. An oral check, on a regular basis is worthwhile. Lift the lips well back and inspect the teeth and gums. Any sign of tartar deposits on teeth, discoloured or sensitive teeth or inflamed gums should be checked out. Your dog may need their teeth cleaned or extractions performed if a tooth is badly infected.
Dental hygiene is often ignored in the dog. The outcome? Consider what your teeth might look and feel like after months, years or even a lifetime of neglect. They would be a wreck, and you would be miserable. Yes, canine teeth also need frequent brushing to prevent gum disease and early tooth loss, as well as just plain foul breath.
Despite the popular conception, dog biscuits and bones do not keep the teeth clean and healthy. Although some veterinarians feel that gnawing on these hard substances has benefit, it does not prevent the build-up of plaque and tartar which, unless removed, can lead to gum inflammation, tooth root abscesses and other oral problems. That’s the simple truth.
The teeth should be brushed at least once or twice a week, more often if possible. As with grooming, acclimation is best started early in the puppy’s life.
To make a toothbrush, fold a square gauze pad loosely around the tip of your index finger. Or you can use a small, soft child’s toothbrush or buy a special toothbrush from a veterinarian. Dip the toothbrush or gauze pad in a toothpaste designed for dogs (not for humans, since human formulations can upset the dog’s stomach) or into a paste made of baking soda and water. Next, vigorously scrub the outside surfaces of the teeth, especially the rear teeth. With the gauze pad, you may also try to gently massage the gums. It is not necessary to brush the interior surfaces of the teeth.
Your veterinarian should check your dog’s mouth for tooth or gum disease during annual checkups. The most common problem, tartar accumulation, resembles yellow or brown cement deposits along the gum line or in the crevices of the teeth. Despite your best efforts, a proper dental cleaning under general anaesthesia may need to be performed periodically in a veterinarian’s office.
Breeder/Exhibitor Ed, Health
BACTERIAL SKIN INFECTIONS (PYODERMAS)
Causes
– Staphylococci (`Staph bacteria´) are the most common organisms found in bacterial skin diseases (pyoderma’s) in dogs. Fortunately, these bacteria (S. intermedius) are not contagious to humans or other pets.
Signs
– Commonly itchy, yellow pustules are often observed early in the disease, and the dog´s skin can be reddened and ulcerated. Dry, crusted areas appear as the condition advances, along with loss of hair in the affected areas (lesions) and an odour.
All areas of a dog´s body may be involved, but most cases are confined to the trunk. The chin is one area commonly affected. Called chin acne, this condition is actually a deep bacterial infection. Obese dogs and dogs of the pug-nosed breeds are frequently affected by pyoderma in the skin folds on their face, lips and vulva.
Other areas where pyoderma may occur include between the toes and on the calluses of the elbows that mostly affects the abdominal area in young puppies.
Diagnosis
– This is usually made from the case history and appearance and location of the lesions. In some cases, it may be necessary to culture the skin (grow the bacteria) and conduct sensitivity tests to determine which antibiotic will be effective in treatment. Most bacterial skin infections in dogs are secondary to another disease such as parasitism, allergies, endocrine (hormonal) disorders or abnormalities in the immune system. Therefore, in recurrent cases, it is important to search for underlying causes. It may be necessary to do blood tests, allergy tests or skin biopsies to achieve a complete diagnosis.
Treatment
– Initial treatments may entail removal of the hair in and around the lesions, washing of the whole dog with antibiotic shampoos such as benzoyl peroxide, careful drying and the application of an antibiotic ointment to local lesions, in most cases, antibiotics will also be administered orally for 3-4 weeks. Bandages or a protective collar which prevents the dog from mutilating the lesions may be applied.
Some pyoderma involving skin folds can require corrective surgery. In recurrent cases where testing reveals no definable underlying cause, special staphylococcal vaccines as an alternative to long-term antibiotic treatment can be tried.
It may be necessary to continue treatments such as antiseptic shampooing, antibiotic ointment applications and giving antibiotics orally at home. While most cases respond to treatment, recurrences of pyoderma are common, particularly if treatment recommendations and follow-up visits to your veterinarian are neglected. Glucocorticoid steroids cannot be administered.
Fungal Skin Infections (Ringworm)
Cause
– The fungal skin infections of dogs are caused primarily be two species of fungi: Microsporum and Trichophyton. The skin diseases resulting from these fungi are commonly called `ringworm.´
Signs
– Ringworm is seen most commonly in young dogs. The fungi live in dead skin tissues, hairs and nails. Hair loss, usually in circular patches, may appear. If infected, the center of the patches may have a dry, crusty appearance. The head and legs are most commonly affected by ringworm, although the disease may spread over other parts of the dog´s body if not treated. Dogs may scratch the lesions.
Diagnosis
– The appearance of the lesions, the history of their development and the age of the dog are all helpful in diagnosing ringworm. A Wood´s Lamp Test (ultraviolet light) can be used to help diagnose the Microsporum species only. A definite diagnosis can be obtained through a fungal culture — grow the fungi found on the affected hairs.
Treatment
– The hair around the lesions is clipped, and special fungicidal shampoos or rinses are used for bathing the dog. Topical lime sulfur and mandatory systemics should be administered.
Public Health Aspects of Ringworm – Ringworm is contagious to humans, particularly to children and to other household pets. Infected dogs should be kept away from children and other dogs and cats until the infection is cures — which can be as long as 2-3 months or more after the treatment begins. Adults should be careful to wash their hands thoroughly after handling an infected dog. If treated early, ringworm is readily controlled in humans. Other household pets should also be examined for ringworm.
Allergic Skin Diseases
Allergies in dogs are common. Signs such as itchy skin, nasal and eye discharges and sneezing, and/or digestive upsets and/or skin lesions may indicate an allergy is present. Many skin diseases seen in dogs are caused by an allergy.
Causes
– An allergy is a hypersensitivity reaction to allergy-causing substances known as `allergens´ or `antigens.´ Dogs (like people) can develop allergies at any age, and the signs can appear quite suddenly.
The most common allergy dogs develop is the flea saliva. The presence of a single flea on these allergic dogs causes intense itching. These allergies are seasonal in climate zones where fleas are eliminated by the cold in winter months — and a year-round problem in warmer climates.
Atopy (atopic dermatitis, allergic inhalant dermatitis) is a pruritic (itchy) skin disease dogs develop in response to inhaled particles such as house dust, molds and pollens. This common form of allergy usually starts at a relatively young age. Rarely, dogs can be allergic to chemicals contained in soaps, waxes, carpets and flea collars. This type of hypersensitivity is known as a `contact allergy.´ Also, some dogs are allergic to insect bites and stings. Food allergies usually case diarrhea and/or skin lesions.
Signs
– Itching is the primary sign of allergic skin diseases in dogs. The affected skin may appear normal, or red and moist in patches called `hot spots.´ Pus and dried crusts are apparent if a bacterial infection is also present. The dog tends to constantly scratch and lick affected areas. Initially, flea allergies are most evident over the dog´s back and near the tail. A dog´s face, feet, chest, and abdomen are more often affected by pollen and dust-type allergies. Contact allergies are seen mostly on the hairless areas of the abdomen and on the bottoms of the feet.
Diagnosis
– The dog´s case history helps with the diagnosis. The intense itching and location of the lesions are also helpful in diagnosing the type of allergy present. Response to treatment (flea control) is often used as a method of diagnosis of flea allergy. Trials of special hypoallergenic diets are used to diagnose food allergy. Allergy testing is used to help choose immunotherapy. Blood tests are also available to diagnose allergies, but their use is more controversial. Ask your veterinarian for his or her current recommendations.
Treatment
– Allergies can be controlled in most cases, with few `cured.´ Antihistamines and corticosteroids may be used by your veterinarian to give your dog relief from the intense itching. In mo
st cases this will stop the self-mutilation. The owner will be instructed to give corticosteroid tablets in decreasing dosages for a few months. Corticosteroids are potent drugs and should not be used carelessly or for long periods of time. The main objective in controlling flea allergies in dogs is to kill the fleas on the dog and in the dog´s environment.
Another approach to allergy control is hyposensitization (immunotherapy). In this procedure, a correct diagnosis by intradermal or blood testing is necessary. The dog is then given injections of small but increasing doses of the allergy-causing substance at varying intervals for up to 12 months. Lifelong response may take up to 12 months.
Parasitic Skin Diseases
Cause
– Fleas are the most common parasitic skin disease found in dogs. Mange is another type of skin disease which is caused by mites. There are two severe types of mange: sarcoptic mange and demodectic mange.
– Ear mites, lice, and ticks are other parasites that affect dogs. Their presence irritates the dog, leading to self-mutilation.
Signs
– Sarcoptic mange causes intense itching, loss of hair and crusting of the skin. A dog´s ears, front legs, chest and abdomen are most often affected by sarcoptic mange.
– Demodectic mange can cause itching. The skin is reddened and scaly, and hair loss occurs in round patches resembling `ringworm.´ The face and front legs are most commonly affected, although some cases may be generalized. Generalized demodectic mange is often a sign of underlying internal disease or a hereditary problem.
– Ear mites cause severe irritation in the ears. Often, an affected dog will scratch the hair off the back of its ears. Ticks, lice and fleas may transmit other diseases, in addition to causing irritation.
Diagnosis
– Mange is often suspected on the basis of the case history and the appearance and location of the lesions. A skin scraping test is always performed to aid in identifying parasites. Ear mites, which are barely visible to the naked eye, appear as small white objects. The black debris commonly seen in the ears of dogs with ear mites is a combination of dried blood, normal ear wax and discharges from inflammation. Lice, fleas and ticks can also be seen by close examination of the dog´s skin.
Treatment
– Mange is treated by clipping the affected areas and washing them with an antiseptic. Anti-mite dips are often necessary and may be used weekly or biweekly for several months. Shampoos can be sued before each dip. The dog´s eyes should be protected with mineral oil or eye ointment and the ears plugged with cotton before dipping. Most cases of mange respond well to this treatment. Antibiotics can be administered in cases of mange where infection may be present.
Ear mites can be readily treated Initially, your veterinarian may recommend a thorough cleaning of the dog´s ears while the animal is sedated. This treatment can be followed up with home treatments using special solutions or ointments to kill the mites and prevent infections in addition, insecticidal dips, sprays, powders or shampoos are often used.
Lice, ticks and fleas must be killed on the dog and in the dog´s environment with insecticides. Dips, shampoos, flea collars, sprays, powders, foams and foggers containing insecticides are available from your veterinarian to help control these parasites.
Hormonal Skin Diseases
Skin diseases caused by hormonal abnormalities in dogs are difficult to diagnose. The thyroid gland, adrenal glands, pituitary gland, testicles and ovaries all produce hormones. If excessive (`hyper´) or deficient (`hypo´), these hormones produce changes in the skin and hair coat. Most hormonal problems that affect the skin produce hair loss that is evenly distributed on each side of the dog´s body. The skin may be thicker or thinner than normal, and there may be changes in the color of the skin or hair coat. These diseases usually are not itchy.
When any of the hormone-producing glands malfunction, they affect other body functions besides the skin. Hormonal skin diseases in dogs can be much more serious than a `skin problem.´
Some causes of hormonal skin disease, such as hypothyroidism and adrenal gland problems, can be diagnosed by special blood tests and effectively treated. Others may be more difficult to diagnose and treat. Skin changes related to the sex hormones can be successfully treated with surgical neutering, if this has not been performed previously.
{supertable table active 0} {active disable} {headrows 1} {headcols 1}{rowheight 1 45px} {rowheight 2 150px} {rowheight 3 150px} {rowheight 4 150px} {rowheight 5 150px} {rowheight 6 150px} {rowheight 7 150px} {rowheight 8 150px} {rowheight 9 150px} {rowheight 10 150px} {rowheight 11 150px} {rowheight 12 150px} {rowheight 13 150px} {rowheight 14 150px} {rowheight 15 150px} {rowheight 16 200px} {rowheight 17 150px} {rowheight 18 150px} {rowheight 19 150px} {rowheight 20 150px} {rowheight 21 150px} {rowheight 22 150px} {rowheight 23 150px} {rowheight 24 150px} {rowheight 25 150px} {rowheight 26 150px} {rowheight 27 150px} {rowheight 28 150px} {rowheight 29 150px}
| Condition |
Description |
Symptoms |
Diagnosis |
Treatment |
| Atopy (Allergic Inhalant Dermatitis) |
Allergic reaction by the animal to something it inhales such as pollen, house dust mites and mold |
Licking of feet, inflamed ears, itching, redness, sometimes development of infection or hot spots |
Intradermal or serologic (blood) testing for allergies |
Reduce exposure to allergen (what the pet is allergic to), shampoos, fatty acid supplements, steroids, antihistamines, immunotherapy |
| Food Allergies |
Allergic reaction to something in the diet |
Licking of feet, inflamed ears, itching, redness, sometimes development of infection or hot spots |
Food elimination trials |
Change in diet |
| Allergic and Irritant Contact Dermatitis |
Reaction of the pet’s skin to something it had contact with such as wool or plastics |
Red skin and small bumps or blisters on the areas of skin that are sparsely haired and directly exposed to the offending substance, itching |
Patch test, exclusion trials |
Restrict exposure to the allergen or contact irritant in the pet’s environment, steroids, antihistamines |
| Flea Allergy Dermatitis (Flea Bite Hypersensitivity) |
Severe reaction by the animal to the saliva of the flea |
Intense itching, redness, hair loss; sometimes development of infection or hot spots |
Presence of fleas; reaction to intradermal testing |
Flea Control in the environment and on the pet; steroids and antihistamines for the itching |
| Sarcoptic Mange |
Infection with the Sarcoptes mite |
Intense itching and self-trauma |
Skin scraping and microscopic examination – the mite is often very difficult to find |
Amitraz (Mitaban) dips (off-label use*); ivermectin (off-label use*) |
| Demodectic Mange in Dogs (Red Mange) |
Infection with the Demodex mite – occurs when the immune system is deficient |
Hair loss, scaliness, redness, pustules, ulcers, sometimes itching |
Skin scraping and microscopic examination |
NO Steroids! Amitraz (Mitaban) dips |
| Cheyletiella (Rabbit Fur Mite) Mange
|
Infection with the Cheyletiella mite |
Itching, scaliness |
Skin scraping and microscopic examination – the mite is often very difficult to find |
Permethrin (Dogs ONLY) or Pyrethrin |
| Ringworm |
Infection with several types of fungus |
Hair loss, scaliness, crusty areas, some itching |
Culture |
Miconazole, lime sulfur dips; oral griseofulvin or itraconazole |
| Yeast Infection |
Infection with, most commonly, Malassezia; usually follows some other underlying disease |
Itching, redness, sometimes oiliness |
Skin scraping/smear and microscopic examination, culture |
Treat underlying disease; oral ketoconazole; miconazole shampoos |
| Hot Spots: Acute Moist Dermatitis |
Result from allergies, flea bites, mange, anal gland disease, poor grooming, ear infections, plant awns or burs, arthritis |
Hair loss; red, moist, oozing skin; constant licking or scratching |
Physical exam and history |
Treat underlying condition; clean area; apply Domeboro solution; topical and/or oral antibiotics and steroids |
| Cutaneous Lymphoma |
Rare type of skin cancer |
Itching, ulcers, nodules, redness |
Biopsy |
Usually does not respond to treatment |
| Lice |
Infection with several species of lice |
Variable; itching, hair loss, crusts, rough hair coat |
Finding lice or nits on skin or hair |
Permethrin (Dogs ONLY) or Pyrethrin, ivermectin (off-label use*) |
| Skin Fold Dermatitis |
Occurs where folds of skin touch each other such as lips, vulva, face (in breeds like bulldogs) |
Redness, oozing, itching |
Physical exam; microscopically examine smear for evidence of infection |
Treat any infections; clean areas daily; surgical correction if severe |
| Hookworms |
Infection with the larvae (immature forms) of hookworms |
Red bumps, usually on feet, rough foot pads, abnormal nail growth, itching |
Physical exam, history of poor sanitation |
Treat for intestinal infection; move animal to different environment |
| Neurodermatitis: Acral Lick Dermatitis (Dogs) Psychogenic Dermatitis (Cats) |
Self-licking in dogs and cats results in self-trauma; possible causes include anxiety, boredom, stress (e.g., new member in household) |
Acral Lick: red, hairless, well-circumscribed lesion usually on forearm; cats: symmetrical hair loss, sometimes ulcers, on abdomen, groin, along the back |
Exclude other causes; history important |
Relieve underlying cause e.g., anxiety; |
| Bacterial Infection |
Often occurs as a result of another condition |
Redness, pustules, bumps, sometimes itching |
Microscopic examination of smear; culture |
Treat underlying condition; topical and/or oral antibiotics |
| Ear Mites |
Infection with Otodectes |
Intense itching of ears, redness, dark crumbly discharge in ears |
Direct visual or microscopic examination of ear discharge |
Clean ears and apply medication containing pyrethrin (Ear Miticide) |
| Pelodera Dermatitis |
Accidental infection with larvae from a non-parasitic worm that lives in straw and other organic material |
Intense itching, redness |
Skin scraping and microscopic examination |
Remove bedding; mild antibacterial shampoo; steroids if necessary to control itching |
| Chiggers (Harvest mites) |
Seasonal disease caused by larvae of the chigger |
Itching, bumps usually on feet, abdomen, folds at base of ears |
Visualization of mite larvae or microscopic examination of skin scraping |
Permethrin (Dogs ONLY) or Pyrethrin |
{/supertable}
Skin medications for dogs include cephalexin, clindamycin, clotrimazole, enrofloxacin otic, gentamicin sulfate, nystatin neomycin sulfate, and thiabendazole.
Breeder/Exhibitor Ed, Health
written by Patti Smith
Both Valerie’s Doberman and mine were diagnosed with Lymphoma. The first step was an accurate diagnosis–I spent a month with 3 different veterinarians trying to find the cause of Nick’s BLACK diarrhea. (Later, I learned, the black color indicated an UPPER gastric problem). An ultra-sound & needle biopsies confirmed gastro-intestinal lymphoma. We were told that rarely does a dog survive over 9 weeks. We were devastated!
A treatment protocol had to be selected, and in Nick’s case, he was put on the “Wisconsin Madison” schedule.
It began with a chemo treatment weekly for 12 weeks; then every other week through the program, then every 3 weeks, and he just ‘graduated’ to every 4 weeks. The one chemo on the schedule, Doxorubicin, can affect the heart function. Because Nick was 3 1/2 at the time, he was treated with the Doxo with no heart protectent. However, after the second Doxo treatment, an ultrasound on his heart showed that his refraction had gone from the normal 50% to 22%. We then gave him the Zinecard (about $550 per vial) before the Doxo was administered. He will not receive any more Doxo.
Having heard of Valerie’s success, Phil & I drove to Las Vegas and spent an afternoon with her. Nick was on Predisone in the beginning stages.
DIET: Carbohydrates feed cancer cells. At first, I did a lot of cooking for him: beef roasts in the crock pot, chicken, broiled salmon, etc. Dr. Hershey had us put him on Wellness Puppy dry meal, and canned Wysong.
I am now also adding Azmira holistic canned/dry. It was difficult to get him to eat in the early stages, but he has a good appetite now. We gave him anything he would eat, including scrambled eggs, high calorie Hill’s Prescription canned food., bacon, etc. Avoid preservatives, color dyes or additives–check labels. Do not buy color-dyed snacks, hooves or pig’s ears. Best snacks are fruits & veggies that have been washed free of pesticides–remember, their immune systems are down from the chemo. Never heat food in microwave as it destroys the enzymes in food & makes your pet’s digestive system work twice as hard to digest the food. Oven baking, broiling, steaming or boiling are best. Always feed 2 meals a day so as not to over-burden the digestive system all at once & allow for a more efficient assimilation of food. Avoid dairy. Sardines in tomato sauce is good for them.
STRESS: all stress was removed from his life. He has his own bedroom with a king-sized bed. There is a small table-top fountain running all the time, and soft relaxation music playing. The color ‘yellow’ stimulates the lymphatic & digestive system, so his room, sheets, are ‘yellow’. It’s VERY calm to sit with him in his room.
EXERCISE: Very limited. He goes outside with no other dogs and we do not encourage him to play or run extensively. Forced rest was suggested by Dr. Hershey.
SUPPLEMENTS:
- Udo Oil Blend
- Ester-C – 2000-3000mg/day
- Pepcid A/C
- Vit E – 800 IU/day
- Selenium – 200 mg/day
- Betacarotene – 50,000 U/day
- B-12 – 500 mg/dayl
- Alpha Lipoic Acid
- Dandelion
- Digestive Enzyme
Valerie also put magnets under the bed — we did not do that. None of us know “what” is working, but we’re sticking with it as the dogs are doing great. In fact, I often ask Dr. Hershey if we didn’t make a mistake in the diagnosis as Nick looks & feels so good. He’s had a wonderful, normal quality of life this past year so it has all been worth it.
I hope this helps — Good luck!
written by Valerie Stanert
Las Vegas, Nevada
submitted by Pat Policastro, Tazzman Dobermans
Phoenix, AZ
Valerie states: My beautiful Daphne is enjoying 4 years in healthy remission this month due to this regimen and we feel very lucky.
NOTE: Here is a tidbit of mine about microwaving: Micro wave ovens use radio waves to excite the water molecules in foods that are being cooked. The water molecules become active thereby heating the food. While it is true that microwaving food kills the enzymes that are naturally present in live/plant foods, the same thing happens when we cook over a stove. The growing myth that microwaving food is somehow nuking it is not based on science but rather uncertainty about how microwaves really work. The name microwave is a misnomer and gives people a sense that some mysterious process is happening to food as its cooked when in fact cooking food by any means kills essential enzymes in food.
Diet and Nutrition Sources:
These are some that I have used, my favourites are marked with an asterisk (*)
- *Strombeck, Donald R. D.V.M. Ph.D. Home-Prepared Dog & Cat Diets. Iowa State University Press. 1999. (This book is an outstanding, highly accessible book that can help you calculate the caloric and nutritional needs of your dog based on his weight, and condition. **Even better is explains why commercial diets are not sufficient for your dog right now (he obviously proposes home prep for all, but the first chapter or so will help you understand why your dog simply cannot benefit from dog food during his illness) There are lots of sample diets, most are for 40lb dogs that you simply double for your dog.)
- *Goldstein, Martin D.V.M. The Nature of Animal Healing. Ballantine Books: New York. 1999. (This book is great, it has a chapter devoted to “taking on cancer” is easy to read and is extremely informative.)
- *Pitcairn, Richard D.V. M. and Susan . Dr. Pitcairn´s Complete Guide to Natural Health for Dogs and Cats. Rodale Press Inc: PA. 1995. (This book is loaded with Information. Pitcairn is extremely well published and respected. This is an outstanding book and usually on the shelves at bookstores and in health food stores.)
- *Brown, Kerry D.V.M. and Volhard Wendy. The Holistic Guide for a Healthy Dog. Howel Book House: New York. 1995. (This book is in my opinion the most scientifically sound Holistic guide that I have read. It has tons of information about alternative treatments and is well organized and easy to read.)
- Billingshurst, Ian B.V.Sc. Give your Dog a Bone. 1993
- Mindell, Earl R., PhD, and Renaghan, Elizabeth. Earl Mindell´s Nutrition and Health for Dogs. Prima Publishing: CA. 1998.
- Brennan, D.V.M., Mary L. and Eckroate, Norma. The Natural Dog: A Complete Guide for Caring Owners. 1993.
Daphne´s Chemotherapy:
Three-drug protocol: Injected vincristine and cyclophosphamide pills to inhibit cell Pision, and prednisone to attack the lymphoma cells.
Sup
plements: ask your Vet or Holistic Vet about:
Enzyme supplements : enzymes help the body break down ingested food so nutrients can be properly absorbed. Enzymes are only in raw food because they are destroyed by heat and therefore can´t survive packaging processes. **When the dog is not eating much or has diarrhea, maximizing absorption is crucial.
One I have used is : PROZYME, www.prozyme.net 1-800-522-5537
I also used an Ester-C product for dogs. You will hear arguments for and against the value of Vitamin C. Dogs do produce some C but you want to support the immune system right now so she needs more. It must be Ester-C– not ascorbic acid, its more absorbable and won´t irritate an already upset stomach. Inter-Cal Nutraceuticals has one. Try www.intercal.com
When choosing diets:
- Some side effects of chemotherapy include bone marrow suppression, bladder inflammation, and liver problems. Try to choose diets from the holistic diets that support these organs. Many of the books I recommended above organize the diets accordingly.
- Boiling makes food bland, Vets recommend it for irritated stomachs and poor appetite, which makes sense. I always keep in mind that vitamins, minerals and enzymes are lost this way.
- I have attached some of the diets I made for Daphne during her Chemotherapy.
- White fish, Chicken, white rice and macaroni are the staples, they are easiest to digest while on the chemo. Notice the diets are higher in protein and slightly higher in fat. In the earlier stages you will want to leave out the extra oil and the salt substitute. Later, the cancer maintenance diet should be higher in protein and fat and lower in carbohydrate, and you can jazz it up with herbs and garlic.
- Sardines in small doses (2 TBS serve two purposes: omega fatty acids, a must and they make the otherwise boring diet irresistible!!)
Daphne (range 1500 -1672 kcal)
AM
3 eggs
1 cup Rice (white)
2 TBS Sardines
2 TBS Veg oil
½ C Tuna
1tsp Bone meal
¼ tsp salt subs
964 kcal 112.1g Protein 49.4g fat
PM
1/3lb Chicken
1 egg
1 ½ c Rice
¼ tsp salt sub
1 vitamin E
553 kcal 46.3g Protein 9.48g fat
1517 kcal total for the day
AM
3 Eggs
2c Rice
2 TBS Sardines
2 TBS Veg oil
¼ tsp salt sub
1 tsp Bone meal
Multi-supp
970 kcal 34.1g protein 49.4g fat
PM
1/3lb Poultry
1 egg
1 ½ c Rice
¼ tsp salt sub
1 vit E
553 kcal 46.3g protein 9.48g fat
AM
½ lb Chicken
2 c Rice
¼ tsp salt sub
multi supp
653 kcal 46.3 g protein 9.48g fat
PM
1/3lb Chicken
2 c Rice
¼ tsp salt sub
575 kcal 40g protein 4.18g fat
Choose Higher Calorie options for AM meal:
½ lb Chicken
2 ½ macaroni
2 TBS Sardines
1 TBS veg oil
1/3 tsp salt sub
Ester -C
1065 kcal 63.6g protein 43.9g fat
3 Eggs
2 c Rice
2 TBS Sardines
2 TBS veg oil
¼ tsp salt sub
1 tsp Bone meal
Multi -supp
964 kcal 34.1g protein 49.4g fat
Choose Lower Calorie options for PM meal:
½ lb Chicken
2 c Rice
¼ tsp salt sub
653 kcal 46.3g protein 9.48g fat
1/3 lb Chicken
2 c Rice
supps
575 kcal 40g protein 4.18g fat
Important! Give B-12 supplement every week! My vet gave me some pre-prepared injectable B-12. Dogs on chemo get weak like people do and they made Daphne feel much better.
Breeder/Exhibitor Ed, Health
James Anable’s site:
Permission granted by Logan Catalfu to post on this site
Remedy for hair loss, especially in blue and fawn Dobermans
B 50 ……………………………………………….. 1 tablet twice daily
Folic Acid 400mcg…………………………… 2 tablets twice a day
Melatonin 1mg ……………………………….. 1 tablet twice a day
Fish Oil 1000mg…………………………….. 1 capsule twice a day
A beautiful blue Doberman with a healthy thick coat
Breeder/Exhibitor Ed, Health
There will always be disagreements about vaccinations and how often one should vaccinate! The articles below are against annual vaccinations. At the bottom of the page are links to vaccination sites which are more complex in their detail and recommend annual vaccinations. I suggest that you read any available material thoroughly and do your own research. Discuss it with your own Veterinarian before making any decisions!
Whilst all care is taken, we will not be held responsible for the accuracy of any information contained on this site. Any errors or omissions will be corrected upon notification. Any articles, statements and opinions expressed on our site are not necessarily the opinion of Chinaroad Löwchens of Australia.
From the AVMA Principles of Vaccination
There is evidence that some vaccines provide immunity beyond one year. Revaccination of patients with sufficient immunity does not add measurably to their disease resistance, and may increase their risk of adverse post-vaccination events. Vaccination is a potent medical procedure with both benefits and associated hazards.
It is not currently possible to determine the immune status of a patient relative to all the infectious diseases of concern without conducting a challenge test. Serology does not predict a patient’s immune status for most diseases. For those diseases where serology has predictive value of a patient’s immune status, the variation within and between laboratories renders the procedure generally unreliable.
Adverse events may be associated with the antigen, adjuvant, carrier, preservative, or a combination thereof. Possible adverse events include failure to immunize, anaphylaxis, immunosuppression, autoimmune disorders, transient infections, and/or long-term infected carrier states. In addition, a causal association in cats between injection sites and the subsequent development of a malignant tumor is the subject of ongoing research. The role of genetic predisposition to adverse events needs further exploration and definition.
Vaccine program goals include providing optimal immunity against clinically relevant diseases the patient is at-risk to contract, while minimizing the potential for adverse events.
…Biological agents are regulated by the USDA, not the Food and Drug Administration, and thus are not subject to those regulations that address extra label use. Veterinarians can legally use vaccines in a discretionary manner.
USDA licensing at the full approval level provides a baseline standard for efficacy, safety, purity, and potency, but the clinical need (relevancy) or usefulness (applicability) of a product are not assured by the licensing process. The USDA must approve labels for biological products. However, current labels frequently contain revaccination interval recommendations based on historical precedence and regulation rather than scientific data, may fail to adequately inform practitioners about optimal use of the product, and the testing methods may be inadequate to identify rare but relevant safety concerns. [2001]
Vaccinations in Veterinary Medicine: Dogs and Cats
By 1996 Don Hamilton, DVM
A practice that was started many years ago and that lacks scientific validity or verification is annual re-vaccinations. Almost without exception there is no immunologic requirement for annual revaccinations. Immunity to viruses persists for years or for the life of the animal. Successful vaccination to most bacterial pathogens produces an immunologic memory that remains for years, allowing an animal to develop a protective anamnestic (secondary) response when exposed to virulent organisms. Only the immune response to toxins requires boosters (e.g. tetanus toxin booster, in humans, is recommended once every 7-10 years). And no toxin vaccines are currently used for dogs and cats. Furthermore, revaccination with most viral vaccines fails to stimulate an anamnestic (secondary) response as a result of interference by existing antibody (similar to maternal antibody interference). The practice of annual vaccination in our opinion should be considered of questionable efficacy unless it is used as a mechanism to provide an annual physical examination or is required by law (i.e., certain states require annual revaccination for rabies).
Summary: Yearly “boosters” are unnecessary, provide no benefit if given (will not increase immunity). Thus boosters are either a legal issue (Rabies) or a manipulation issue (inducing clients to come in for examination rather than directly suggesting an examination).
The issue of initial vaccination is less clear than that of boosters. Many clinicians feel that without vaccination they would see outbreaks of disease, particularly canine parvovirus disease. This can be a difficult issue to resolve. A fundamental dilemma is that vaccination in effect leads to weakening of the gene pool, and thus the overall health of a given population. One way this occurs is by allowing individuals to live that would otherwise succumb to disease, such disease being a natural means to “cleanse” and thus strengthen that population. This naturally presents an ethical quandary these days (our understanding of native or aboriginal thinking suggests that letting weak individuals die was implicitly understood to be not only acceptable but proper). Western society values the individual’s right to be, therefore we make efforts to save all individuals. Any answer to this question naturally lies with the individual(s) involved. The second, and more compelling theory of the mechanism of interaction between a vaccine and the body suggests that vaccines “protect” against the acute disease not by preventing the disease but by changing the form of the disease to a chronic disease. 2 For example, the panleukopenia virus of cats induces an intense, rapidly progressive malfunction in the digestive tract, leading to vomiting and/or diarrhoea. In adult vaccinated animals this translates into a chronic state of diarrhoea and sometimes vomiting. This disease is known as inflammatory bowel disease (IBD), an autoimmune disease of the intestines. IBD has been occurring at near epidemic levels over the past several years; no other reasonable explanation has been proposed for the proliferation of cases of the disease. Vaccinations are known to be a major trigger of other autoimmune processes in susceptible individuals, 3 so it is reasonable to suspect vaccines as a trigger for IBD. Another aspect of panleukopenia virus infection, implied by the name of the virus, is vastly lowered numbers of white blood cells and corresponding immune deficiency. Could the appearance of Feline Leukaemia virus disease and later Feline Immunodeficiency virus disease be related to vaccination for panleukopenia during the previous two decades? The logicality of this theory does not allow easy dismissal of a relationship, most likely cause and effect. Both of the latter diseases produce low white blood cell counts and immunodeficiency as part of their symptom complexes. Similar connections have been proposed between Canine Distemper virus disease and both kennel cough and Canine Parvovirus diseases as “distemper” includes a pneumonia component as well as severe diarrhoea. Chronic coughing is characteristic of kennel cough; parvovirus disease affects the intestines, producing severe diarrhoea and vomiting. Additionally, the incidence of inflammatory bowel disease in dogs appears to be on the increase in the past year
or two. Vaccination of dogs for Canine Parvovirus has been in effect for fifteen years, contrasted with the much longer history of parvovirus vaccination in cats (Feline Panleukopenia virus is a member of the parvovirus family). This portends a frightening future for dogs if the connection is indeed correct. Finally, connections are proposed between vaccination for Rabies and increasing numbers of fearful, aggressive animals. Behavioral problems of the extent seen today are a recent occurrence, being rare only two to three decades ago. 4 Their emergence is coincident with the practice of repeated adult vaccination, suggesting the need to examine that relationship. Aggressive behavior has been observed in dogs for several days following vaccination for rabies, even with non-infectious [killed] vaccines.5, 6
As practitioners sharing responsibility for the well being of patients, veterinarians are faced with a challenge when dealing with acute diseases. Vaccinations may prevent these acute diseases, but if the exchange is for a lifetime of chronic disease, is that a viable option? (Viable is from the French vie, meaning life, so the question is will the patient live and flourish or simply exist.)
First, remembering that booster vaccines are unnecessary, we can stop all vaccination after one year of age for virtually all diseases. (cf. below; Rabies is required by law so we need to work to change the laws so that they are in accordance with the fact rather than fear.) As repetition naturally increases the likelihood of problems, we can reduce side effects tremendously with no additional risk to the patient, simply by stopping adult boosters. Of course, there will still be some risk involved with even the initial vaccinations, but no risk of contracting the acute disease once the animal is immunized by these first vaccines. See below for duration of immunity to the various diseases for which vaccines are available.
Secondly, all vaccines should be administered as single antigens. (An antigen is something that is capable of eliciting an immune response, in this case a viral or bacterial organism from which a vaccine is produced.) This means not using the polyvalent vaccines which have become so common these days. Natural exposure to diseases is usually one at a time, and the body is probably more successful at responding to only one antigen and producing immunity without adverse effects, rather than responding to a complex of antigens. Therefore, rather than giving a group of antigens together at three to four week intervals, individual components should be given using an alternating schedule with a minimum of repetition. (Cf. below)
Thirdly, only immunize for diseases which meet all of the following criteria:
1. The disease is serious, even life threatening.
2. The animal is or will be exposed to the disease.
3. The vaccine for the disease is known to be effective.
4. The vaccine for the disease is considered safe.
Let us take Feline Leukaemia virus (FeLV) disease as an example. An indoor only cat will not be exposed as this requires direct, intimate, cat-to-cat contact. Many veterinarians recommend immunizing indoor cats against this disease. I feel this is unethical. This disease does not fit criteria number three or four anyway in my experience, so vaccination is unwarranted in most if not all circumstances. Feline Infectious Peritonitis (FIP) virus disease is another disease which fits neither three or four. FIP vaccine has generally been found ineffective and has produced severe side effects. Among the side effects I have observed with both FIP and FeLV is induction of the clinical disease they were intended to prevent. In dogs, Canine Hepatitis (CH) virus is almost nonexistent (the vaccine virus to prevent CH is Adenovirus-2). Leptospirosis is extremely rare and often not the same serotype used in the vaccine 7 and the bacterin for “lepto” is very prone to side effects. Coronavirus disease was never a serious threat except to dog companions’ bank accounts, the same being true for Lyme disease except possibly in very small regions. Kennel cough disease is generally not serious (criteria one), and one study showed immunization to be ineffective or even counterproductive. 8 Immunization should be limited to high risk circumstances, if at all. A similar situation exists with the feline upper respiratory diseases; most are not serious except in very young kittens who contract the disease before vaccines are typically administered. Rabies is another disease for which indoor cats and well confined dogs have no exposure, so the vaccine is clinically unnecessary although required by law.
Fourth, vaccines should NEVER be given to unhealthy animals. This is a practice that is gaining popularity among veterinarians for some strange reason, and it goes against the recommendations in all vaccine inserts as well as those of virtually all immunologists. This is malpractice in my opinion.
A bolder option is to refuse immunizations entirely, recognizing the inherent risk in administration of even one vaccine into the body, and being willing to accept the risk of not immunizing. While risk does exist if animals are unvaccinated, it can be moderated significantly by feeding better quality foods (home prepared, including fresh, raw meats) and by limiting exposure until the animals are six to eight months of age. An unvaccinated animal will be significantly less likely to suffer from allergies and many health problems. Skin allergic reactions have been associated with vaccine administration, 9 and tremendous numbers of dogs and cats have skin allergies today. Some other diseases for which links to vaccines are known or suspected include epilepsy, thyroid disorders 10 (hyper- and hypothyroidism), chronic hepatitis, renal failure, cystitis or lower urinary tract disease (particularly in cats), autoimmune hemolytic anaemia, 11 neurologic diseases such as confusion and inability to be “present”, asthma, and so on. In humans sudden infant death syndrome is strongly linked to DPT vaccination, 12 as are attention deficit disease/hyperactivity and autism, 13 among many others including severe brain damage.
Why are vaccines worse than natural exposure? Probably the major factors are the artificial means by which exposure is created with vaccines and the repetition. With few exceptions (primarily rabies and occasionally Feline Leukaemia virus or Feline Immunodeficiency virus), infectious organisms are transmitted via oral and nasal exposure, and this response begins at the oral/nasal level with recognition of a foreign material or organism, followed by initial non-specific destruction and elimination of the organism at the local site of exposure as well as within the blood stream whence an organism may not even reach the interior to cause deep illness, but may be successfully repelled at the periphery. In other cases the body would have a lag time of several hours or even days to begin mounting a response before the “invader” reaches interior organs. As a consequence, deeper pathology may be minimized or even averted. This interior organ pathology may be a direct result of the organism, or it may be an indirect result, manifested through antigen-antibody complexes or other immune system components. These components may inadvertently damage body tissues as “innocent bystanders”, or may directly attack or invade tissues due to recognition problems (autoimmune diseases). The latter may happen because of similarity between organism structures and host tissues; often this involves the nucleoproteins (DNA or RNA), molecules that are important for controlling activity at a cellular level.
When a vaccine is administered, the organism is injected direc
tly into body tissues, bypassing the local immune responses. When this happens, much of the immune system is rendered useless. The body then must compensate by increasing the activity of the balance of the system, and the defences begin in a compromised state, with the organism already in the blood stream. Within the blood stream, the primary aspects of the immune system are antibodies, proteins which attach to the organism and assist in its destruction. Although normally only a part of the defences, these antibodies become heavily responsible in a vaccine (injected) induced invasion, thereby initiating a hyperactive (increased) response. Additionally, the preparation of vaccines often breaks down the integral structure of the virus or bacteria, exposing internal strictures such as viral DNA or RNA (depending on the virus) to the immune system, leading to heavy antibody production against these nucleoproteins. Since nucleoproteins are relatively similar in all life forms, the host antibodies may lose the induced hyperactivity of antibody production. The result may be antibody mediated destruction of host tissue, and autoimmune disease. In a natural exposure, antibodies would be directed more at external structures, which are less similar to host tissues thus less likely to induce cross reactions. Incidentally, autoimmune diseases are occurring more frequently than ever; could this be a reason?
Aside from the above considerations, vaccines commonly contain materials other than the organism to which immunity is desired. These materials may be added as preservatives, adjuvants (materials to stimulate immune response, usually added to non-infectious [killed] vaccines), or antibiotics. Preservatives and adjuvants include such toxins and carcinogens as aluminum (alum), mercury (thimersol), and formaldehyde. Also, many foreign proteins are included if the organism was grown on foreign tissue such as chicken or duck embryos. Even more frightening, non-intended organisms are sometimes accidentally incorporated as contaminant “stowaways”. In 1995 The Washington Post reported that MMR vaccine produced by Merck & Co. along with some influenza and yellow fever vaccines, contained an enzyme known as reverse transcriptase. This enzyme is associated with retroviruses such as FeLV, FIV, and HIV, and has the capability to alter genetic information, leading to serious diseases such as leukaemia and other cancers. These diseases may take years to manifest, so correlation with vaccination may be impossible, masking a potentially causative relationship.
The recommended schedules (age to vaccinate) are from Dr. Schultz, with a few changes as follows: He supports the use of combination vaccines and I strongly do not. He thus recommends in cats to combine Panleukopenia (FPL), Calicivrus (FC), and Rhinotracheitis (FVR) in one schedule; I have recommended to use FVR-FC intranasal vaccine only if needed, and separately from FPL. In dogs he would combine Distemper (CD), Parvo (CPV), and Hepatitis, and possibly Corona and Parainfluenza. I would recommend CD and CPV only, and not combined.
I generally support the use of killed (non-infectious) vaccines, as I feel they have less likelihood for long term damage, but Dr. Schultz presents a strong case for the use of modified live vaccines (MLV) as repetition can be necessary with non-infectious vaccines. With MLV, one dose can have high efficacy. This primarily applies to DC and CPV as non-infectious [killed] Rabies and FP are as effective as MLV. Dr. Schultz’ one dose-95% (one dose of vaccine at a given age will successfully immunize 95% of animals) suggestions are as follows.
Canine Distemper (MLV) 10-12 weeks
Canine Parvovirus (MLV) 12-14 weeks
Feline Panleukoenia (non-inf. [killed] OK) 10-12 weeks
Finally, a comment about vaccinations and choice. While the concept of ‘owning’ an animal is one with which I am uncomfortable, I do recognize that this is how the human-animal relationship is $@%#*ed from a legal perspective. Otherwise we certainly can be said to be guardians of our companion animals. Within this framework the choice about vaccination rests with the human who has accepted responsible guardianship. It does not rest with the veterinarian. Another trend of the past few years is coercion of guardians into procedures such as vaccination. This coercion may be blatant, such as refusal to provide services, even emergency care, unless the animal is ‘current’ on vaccines. Sometimes even critically ill animals are vaccinated upon admission for treatment. More subtle means include induction of fear and/or guilt by asserting (as an authority figure) that companion animals are at risk if not vaccinated yearly, and that failure to comply is evidence of lack of caring. Tactics such as this can create feelings of guilt in the guardian, leading to a fear based decision to vaccinate an animal that is not at risk. This is unethical if not outright malpractice and refusal is an acceptable response. As has been stated above, rabies vaccination is legally compulsive at one to three year intervals, so refusal is a legal risk. Fighting to change these laws, however, is appropriate.
Footnotes
1 T.R. Phillips, T.R., DVM and Ron Schultz, PhD, Canine and Feline Vaccinations in Current Veterinary Therapy, Volume XI Robert Kirk, DVM and John Bonagura, DVM, eds., 1992.
2 Pitcarin, Richard, DVM, PhD, A New Look at the Vaccine Questions. Proceedings of the American Holistic Veterinary Medical Association, 1993.
3 Dodds, W. Jean, DVM, More Bumps on the Vaccine Road, Proceedings of the American Holistic Veterinary Medical Association, 1995.
4 Young, Arthur, DVM, Personal communication.
5 Blanco, B. Dee, DVM, Personal communication.
6 Hamilton, Don, DVM, Personal observation.
7 Schultz, Ronald D., PhD, American Holistic Veterinary Medical Association Annual Conference, 1995.
8 Day, Christopher, E.I., MRCVS Isopathic Prevention of Kennel Cough – Is Vaccination Justified? International Journal of Veterinary Homeopathy, Vol. 2, number 2, 1987.
9 Scheibner, Viera, PhD, Vaccination: The Medical Assault on the Immune System, Australian Print Group, Maryborough, Victoria, Australia, 1993, p. 21.
10 Dodds, 1995.
11 Ibid.
12 Scheibner 1993.
13 Coulter, Harris, PhD, Vaccination, Social Violence and Criminality, North Atlantic Books, 1990.
Copyright 1996 Don Hamilton, DVM
Please feel free to copy and disseminate this article, however it must be copied exactly (with no changes) unless written permission is obtained from the Dr. Hamilton.
Should You Really Be Giving Your Dog or Cat All Those Shots?
by Gene Franks
When Mary Phillips’ dog Peanut died following a routine rabies shot, Mary, who lives in Liverpool, NY, started looking into the ailment listed by the veterinarian as the cause of death. Autoimmune hemolytic anaemia (AHA), she learned, causes the body to attack its own red blood cells. A Cornell University researcher attributed the condition to “chemical or toxic agents or immune-mediated destruction.” Merck’s Veterinary Manual more specifically states that “exposure to live parvo vaccine may be the initial cause in canines.” The rabies vaccine box itself, which apparently no one ever reads, warns: “Tissue-origin vaccines contain extraneous protein in addition to rabies antigen that can lead to autoimmune disease.”
Mary’s research led her to the realization that many veterinarians are very much aware that the vaccinations they routinely give can cause significant harm to animals. She found that there is even a name, vaccinosis, which is used to
describe the chronic illness that results from vaccination. According to Dr. J. Compton Burnett, MD, “Vaccinosis is to be understood as the disturbance of the vital force by vaccination, that results in mental, emotional and physical changes that can, in some cases, be a permanent condition.”
Research into animal vaccines led Mary to an article in the May, 1995 issue of Wolf Clan magazine. Several veterinarians were asked by the magazine to comment on problems associated with routine animal vaccines. I think you’ll be surprised at their candor. It is obvious that vaccines, the bread and butter of the veterinary practice, are held in low esteem by many in the profession. The following comments were excerpted by Mary Phillips from the Wolf Clan article and published in the Spring 1996 issue of The Civil Abolitionist. Here are some things the veterinarians and medical doctors had to say:
The first thing that must change with routine vaccinations is the myth that vaccines are not harmful…. Veterinarians and animal guardians have to come to realize that they are not protecting animals from disease by annual vaccinations, but in fact, are destroying the health and immune systems of these same animals they love and care for.
Dr. Charles E Loops, DVM, Pittsboro, NC.
Injected vaccines bypass normal defences. They implant mutated micro-organisms, preservatives, foreign animal proteins and other compounds directly into the system. This is done in the name of preventing a few syndromes. If an animal is in an optimal state of health, he or she will produce the strongest immune response possible. This response offers protection against all natural challenges. The irony is that vaccine labels say they are to be given only to healthy animals. If they were truly healthy, they would not need them. Those who are not healthy are the most severely damaged.
Dr. Russell Swift, DVM. Ft Lauderdale FL.
Vaccinosis is the reaction from common inoculations (vaccines) against the body’s immune system and general well being. These reactions might take months or years to show up and will cause undue harm to future generations.
Dr. Pedro Rivera, DVM, Sturtevant WI.
In a general and frightening context, I see the overall health and longevity of animals deteriorating. The bodies of most animals have a tremendous capacity to detoxify poisons, but they do have a limit. I think we often exceed that limit and overwhelm the body’s immune system function with toxins from vaccines.
The most common problems I see that are directly related to vaccines on a day to day basis are ear or skin conditions, such as chronic discharges and itching. I also see behavior problems such as fearfulness or aggression. Often guardians will report that these begin shortly after vaccination, and are exacerbated with every vaccine.
Dr. Pat Bradley, DVM Conway AZ
If an animal already has problems, those problems are contributed to by vaccines. So I don’t want to give any more (shots).
Dr. Michael Lemmon, DVM, Renton WA.
Routine vaccinations are probably the worst thing that we do for our animals. Repeating vaccinations on a yearly basis undermines the whole energetic well-being of our animals. Animals do not seem to be decimated by one or two vaccines when they are young, and veterinary immunologists tell us that viral vaccines need only be given once or twice in an animal’s life. First, there is no need for annual vaccinations, and second, they definitely cause chronic disease.
Dr. Christina Chambreau, DVM, Sparks MD
Unfortunately our society is in the grasp of a health panacea and this panacea is fuelled by the biomedical and pharmaceutical industries. Vaccinations have become the modern day equivalent of leeching. First of of all, introducing foreign material via subcutaneous or intramuscular injection is extremely upsetting to the body’s defence system. In response to this violation, there have been increased autoimmune disease (allergies being one component), epilepsy, neoplasia (tumors), as well as behavioral problems in small animals. Even though man and animals have been around for thousands of years, interestingly, the increase in cancer, respiratory disorders (most air quality standards are higher today than in decades past.), and autoimmune problems have likewise escalated alarmingly during the previous decade. Vaccines are not the only culprit for these increases; however, I feel they are one of the primary offenders.
Dr. Mike Kohn, DVM, Madison Wl
Vaccines are not always effective, safety is unproven, and long term consequences are unknown. Despite this, the government requires their use, resulting in a lack of incentives for drug companies to produce better products. Additionally, mandatory vaccine laws make it impossible to conduct properly controlled studies, so we’ll never know if vaccines are truly safe, as is claimed by the government and medical profession. Similar to other procedures, the right of informed consent, i.e. the right to say ‘NO’, should apply to vaccines.
Dr. Kristine Severyn, RPH, Ph.D., Director Ohio Parents for Vaccine Safety .
I believe that vaccinations, especially the rabies vaccines, are contributing to a lot of the “allergic” skin problems seen today, leading to a problem known as vaccinosis, which is characterized by itchy, dark, thickened skin; especially over the abdomen and under the legs. It is seen in both dogs and cats, but is more obvious in the dog.
Dr. Ana Maria Scholey, Holistic Veterinarian.
I think we eventually have to take a look at what is happening to animals because of repeated vaccinations. If you have an animal that within 10 days from the time he received vaccines falls back into a condition that you’d been trying to clean up for some time, you know what happened. We’re seeing a condition that is being described by some of my colleagues and myself as vaccinosis. We have to recognize it as being there.
Dr. Norman C. Ralston, DVM, Mesquite, TX.
The idea of annual vaccines is really questionable. There is no scientific basis from what I’ve been able to read. There was a good article in Current Veterinary Therapy a couple of years ago. They did a literature search and the two authors were not ‘alternative’ veterinarians, and they could find no scientific basis for annual vaccines. So it’s just being done; there is no real basis for the practice. There are a lot of chronic conditions that develop some time after vaccinating. Some of these conditions that I see are chronic ear infections, digestive problems, seizures, skin problems, and behavioral problems.
Stephen R Blake, DVM, San Diego, CA.
Every time a dog is vaccinated for parvo, the number of white blood cells in the circulation decreases for a while. This means their immune system won’t work as well during that time. Every veterinarian who has been in practice long enough has seen reactions to vaccines, ranging from lethargy, mild fever, sore neck, to vomiting and sleeping for 24 hours, to total collapse and shock. In cats we now recognize that this in time can cause fibrosarcoma, a nasty cancer. This is officially recognized by the veterinary community, and if this isn’t a form of vaccinosis, I don’t know what is.
Dr. Nancy Scanlan, DVM, Chino Hills CA
Article extract from Purewater Gazette
It is reasonably certain at this time that distemper and parvovirus vaccinations have a duration of effect of at least three years and
probably closer to five years, with the probability that at least some dogs have lifelong immunity after the initial vaccination series and the one year booster. The adenovirus portion of the vaccine is also reported to have a long duration of immunity and I am not certain about parainfluenza but I also do not consider this to be a very important virus to protect against. So, at the present time we are in the process of deciding what vaccine interval we will use for dogs over the next few years.
I do not see much value in running titers to assess the immune system status against the various viral illnesses which there are vaccines for. High titers are not necessarily a sure sign of protection and low, or even absent titers, do not mean that there is not protection remaining due to the presence of active memory cells still programmed to recognize the virus the vaccine is supposed to protect against. The best test to determine immunity is a virus challenge but nobody in their right mind wants to use this standard to determine the protection for their individual pet.
So at present, I think that the best approach is to use a reasonable time interval between vaccinations based on available information on duration of immunity. We will probably go to three year intervals in our practice, as a reasonable compromise between yearly vaccinations, which do not seem necessary, and taking the risk of loss of protection as a patient approaches the average time that protection is known to decrease.
I do think that it is important to continue to have yearly physical examinations because pets do not communicate illness well, in many instances, and because things like ear infections, dental problems, cataracts, etc. are hard for many owners to detect but are detectable by someone who knows what to look for.
Mike Richards, DVM
Web Site
As the American Veterinary Medical Association states: “Veterinarians must
promote the value of the exam and move away from their dependence on vaccine income.”
Breeder/Exhibitor Ed, Health
written and submitted by Bonnie Dunlop, Botrina Kennels
Twelve Essential Oils For Animals
Any of the following oils or their hydrosols (flower waters) may be appropriate for use with your pet. However, DO NOT apply full-strength essential oils.
1. Basil (ocimumbasilicum) or French Basil, also referred to as common basil, has a colorless or pale yellow hue which is has a light, sweet, fresh, spicy fragrance. It is an anit-depressant, antiseptic, anti-spasmodic, gas reliever, digestive aid, expectorant (meaning it helps remove mucus congestion from the lungs), fever reducer, nerve tonic, adrenal cortex stimulant and general tonic. It stimulates milk production in nursing mothers, treats respiratory infections (when applied to the skin or fur), helps relieve arthritis pain (when applied to joints and muscles), treats indigestion/nausea and flatulence (when taken orally – by mouth), and in all applications it helps relieve depression/fatigue and insomnia.
Exotic basil is NOT recommended for use in animals either externally or internally.
All basil oils should be avoided during breeding and pregnancy.
2. Bergamot (Citrus bergamia)
Bergamot oil is distilled from the rind of an Italian citrus fruit and should not be confused with bee balm (commonly called bergamot)
It is used to treat fevers and worms. This oil has analgesic or pain-relieving, antiseptic , antispasmodic, antitoxic, gas-relieving, digestive, diuretic, deodorant, laxative, stimulant, tonic and worm killing properties. Can be used as an appetite stimulant for anorexia. Taken internally it can help clear bladder infections.
Bergamot oil applied topically should be greatly diluted as it can make bare skin photosensitive.
3. Chamomile (Matricaria chamomilla, known as German true or annual chamomile, and Anthemisnobilis, Roman or perennial chamomile)
The oil of annual German chamomile is thick and blue with an intense, sweet herbal fragrance. The oil of perennial Roman chamomile is clear and yellowish-green with a sweet, clean, fruity odor.
Chamomile is an anti-inflammatory, pain-relieving, antispasmotic, gas-relieving, fever-reducing, antiseptic, wound-healing digestive aid and calming herb of the highest order. Used to treat burns, cuts, infections and abscesses when applied topically. Used for colitis, intestinal infections, gallbladder problems, colic, flatulence and gastritis when taken internally or orally. It makes a spirit-lifting air freshener when sprayed in the air. It is safe for puppies and nursing mothers as well as during pregnancy. Its calming influence relieves tension, depression and anxiety. When put in shampoos and conditioners, it improves coat condition while highlighting red, yellow and light coloured coats.
4. Cinnamon Oil (Cinnamomumzeylanicum and other species)
It is extracted by steam distillation from the leaves, twigs and dried inner bark of the tree. The oil is pale to dark yellow or brown oil and has the familiar cinnamon odor.
The leaf oil is relatively non-toxic, though should be used in moderation around mucous membranes. The bark oil is a serious irritant to the skin as well as mucous membranes. It should not be used during pregnancy, labor or whelping. It is safe for internal use. Used externally for repelling lice and other small parasites. Diluted cinnamon oil warms and relaxes arthritic muscles and joints. Internally it stimulates appetite, helps prevent colitis and heals intestinal infections. As a spray (in the air), it helps improve circulation and boosts the immune system. Freshly ground cinnamon can be added to pets food.
5. Clary Sage (Salvia sclarea) is a close relative of garden sage. Garden sage (salvia officinalis) is toxic in very small doses and should NOT be used in or on animals.
Clary sage is much milder and has a reputation as an aphrodisiac. It may be used in a spray on or around dogs during breeding. It is also used as an antidote to the stress of travel, competition and performing.
6. Clove (Eugenia caryophyllata, E. Aromatica, E. Caryophyllus) does more than numb the gums. As an effective antiseptic, it can be applied to infected wounds and when diluted to 1 percent, clove oil is up to 4 times more effective than phenol in killing bacteria. It is an effective insect repellent, can be used on herbal flea collars or added to herbal sprays. Orally or internally, it helps prevent flatulence, digestive problems and diarrhea. It is an effective vermifuge or worm killer. It is thought or was thought to strengthen the uterus and aid in whelping.
There are three types available : clove bud, clove leaf and clove stem. All three can cause skin irritation and mucous membrane irritation so should be well diluted if used topically. Clove bud is the least toxic. All three are safe for internal use.
7. Eucalpytus or Blue Gum ( Eucalyptusglobulus). The oil is colourless, but turns yellow with age and has a harsh, woody, camphor smell. Externally it is non-toxic and when diluted won´t irritate the skin, but it CAN be toxic if swallowed. Less than a teaspoon can be fatal to a human.
8. Lavender( lavandulalatifolia or spike lavender; L. Angustifolia or L. Officinalis, true lavender; and Lavandula x intermedia or lavandin, a cross between true and spike lavender)
All the different lavenders share the same basic actions: analgesic or pain-relieving, anticonvulsive, antidepressant, antimicrobial, antirheumatic, antiseptic, anti-spasmotic, antitoxic, gas-relieving, bile-stimulating, deodorant, diuretic, insect-repelling, relaxing, circulation-stimulating, tonic and worm-repelling. It is also effective in treating burns and scalds because it neutralizes the venom of insect bites and stings as well as some venomous snakes.
Distilled lavender oil is clear or pale yellow with a sweet, herby, woody scent. It treats respiratory conditions when inhaled or ingested; relieves nausea when taken orally; prevents flatulence , helps alleviate cramping, improves digestion and clears urinary tract infections, ringworm, lice, scabies, sores, sunburn, dermatitis, earache, wounds and inflammation. It relieves anxiety and lifts the spirits. It is safe for dogs of all ages.
9. Myrrh( Commiphoramyrrha and other species)
The essential oil is steam- distilled and acts as an anti-inflammatory, antimicrobial, antiseptic, astringent, gas-relieving, expectorant, sedative, fungicidal and revitalizing. It has a spicy, medicinal odor that stimulates the lungs. Ringworm and other fungal infections respond to preparations containing Myrrh. It should be well diluted.
10. Orange ( Citrusaurantiumvar, amara, or bitter orange, and Citrus sinensis, or sweet orange)
Both bitter and sweet orange oils are called phototoxic because treated skin reacts to sunlight, producing a rash or burn.
Orange flower or neroli oil has a light, sweet, floral fragrance and is used as an antidepressant, antispasmotic, deodorant, gas-relieving, and mild sedative. It is a cardiac tonic, digestive aid and antiseptic. It is neither toxic, irritating, sensitizing nor phototoxic. It can be applied to pet´s scars or wounds to stimulate healing.
11. Sandalwood( Santalum album)
Its pale, viscous (thick) essential oil has a distinctive, soft, sweet, balsamic fragrance and is nontoxic, nonirritating and nonsensitizing. It is well tolerated by people and animals just like Lavender and Chamomile, even at full strength. Applied topically, it helps heal dry, cracked, chapped skin. It can be used to treat a greasy coat or skin. It relieves nervous tension and encourages restful sleep.
12. Tea Tree or Ti Tree( Melaleucaalternifolia)
Because of its unpleasant taste, some pet guides recommend using it to apply to the body parts of an animal that chews or licks incessantly. High concentration or over use on an animal can cause a toxicosis with symptoms such as depression, weakness, incoordination and muscle tremors. The symptoms can start within 2 to 8 hours of application and take 3 to 4 days to subside. It is not recommended for internal use.
Breeder/Exhibitor Ed, Health
by Margi Bragg, ADPEF Historian www.adpef.org
Reprinted with permission obtained by Marj Brooks
PART 1:
A consideration of the consequences to a breed of having but a few genetic founders.
Reprinted from 1999 Doberman Quarterly, with permission from the author
One of my “sub-hobbies” in Dobermans has been tracing pedigrees back as far as possible. I´ll admit that I didn´t initially undertake this to educate myself, I just like to know where pedigrees lead and I find it enjoyable in itself. However, there came a point when I realized that I was acquiring some profound insights into the history of the breed and that these insights apply to today´s Doberman in ways that affect us all.
Most students of the breed know that Dobermans are just now one hundred years old. We are very lucky in one sense, because we are one of a very few breeds that can know our whole history. On the other hand we cannot assume that our breed is “finished” at such a young age. Many of the so-called “ancient” breeds, such as Pharaoh Hounds, have far fewer genetic syndromes, probably because the breeders of long ago wouldn´t support a dog that was non-functional. Within the entire history of the Doberman, he has been a pet and show dog far more than he has been a true working dog. To a large extent, we have not only circumvented the process of natural selection, but even the process of functional selection (at least as far as the ability to perform the breed´s work, as originally conceived) for more than fifty percent of our breed´s entire history. As a direct result, I believe that we are now facing a genetic crossroads in the Doberman that will determine if our breed survives another hundred years.
About ten years ago I began to wonder if my knowledge of old pedigrees could help me understand what has happened in the Doberman. How did we arrive at such a point of gene saturation in a mere hundred years? Most Doberman pedigrees go less than twenty generations deep to end up at the first registered dogs. In comparison with “older” breeds, this seems barely enough time to create a breed at all, and definitely not enough time to arrive at the kind of consistency we take for granted and certainly expect of our show litters. This gave me a clue that I was looking for: A very small gene pool in the origins of our breed. I began to look at the old pedigrees with new eyes. And what I found was even worse than I expected.
One of the prerequisites of a gene pool, be it Dobermans or cheetahs, is that it must have enough genetic variability to allow some members to survive even if most of the group acquires a genetic defect. Now this is an oversimplification to be sure, but the ultimate enemy of isolated natural populations is usually inbreeding. As inbreeding rises, genetic variability falls, eventually allowing the group as a whole to become afflicted with some genetic defect that precludes reproduction or survival of the offspring…. Hello, extinction! This class of genetic defect must be mentally separated from the diseases of old age, which only affect the organism after it has reproduced. Every gene pool has its share of genetic detritus, which affects (reduces) longevity, but if an organism carrying such genes has produced viable offspring before the genes´ lethality/morbidity becomes active, then the offspring too, will have acquired -and will pass along those genes. When I began looking into the history of Dobermans…the produce of a mere three breedings – represented by only five dogs -came to dominate the entire breed over the next ten years…it was at once apparent to me that the “breed” began to be consistent and show dramatic improvement in type almost immediately. Within fifty years we begin to see in photographs a dog very similar to today´s dog. We don´t know the exact numbers of foundation stock, as some were unregistered, but we do know that the breed was begun with relatively few specimens. Between 1900 and the first world war (1914), the breed proliferated greatly, and the gene pool was even enlarged with the influx of new genetic material, e.g. the black greyhound cross Stella, whelped 1908, and two crosses with the Manchester Terriers – first about 1902 and then, again, in 1908. World War I gravely reduced this original gene pool, and the remnants again proliferated until just before World War II (1939).
In America, the first recorded Doberman arrived in 1908 and the breed also sailed along here. However, the really pivotal occurrence came almost fifty years into the Doberman´s history, and it is from the point of World War II (1939-1945) that we have been heading for a crisis with the Doberman. In Europe, the crisis is more understandable, because the breed and breeders both had to pick up the pieces of lives and a gene pool. In America what happened can´t be explained so easily, because the crisis was precipitated not by the war, but by the exact same decision making process that we, as breeders, are still using today -Success breeds Success.
Prior to WW II, America had a huge population of Dobermans and after the war that population came to represent almost the entire gene pool of Dobermans. Since the number of individuals was relatively large, the effects of decreased genetic variability might seem remote. However, the produce of a mere three breedings – represented by only five dogs – came to dominate the entire breed over the next ten years, to the degree that it can truly be said that these five dogs, all born in the decade of the 1930´s, are virtually all there is in a modern pedigree.
I have observed, when one traces a pedigree back far enough today, nearly every line of every pedigree will end up at one of the following three breedings:
- Blank vd Domstadt x Ossi v Stahlhelm
- Kurt vd Rheinperle-Rhinegold x Jessy vd Sonnenhoehe
- Kurt vd Rhineperle-Rhinegoldx Gretl v Kienlesberg.
Occasionally, we can also find Pericles of Westphalia (Kurt´s son) x Jessy. Only in the rarest of circumstances do we find a cross out to any other (unrelated) bloodline that predated these dogs. When one considers that in a fifteen generation pedigree there are possibly 16,384 distinct individuals in the fifteenth generation alone, to accept that the above handful of matings may appear repeated upwards of 8000 times is usually more than anyone can believe.
In fact, when I discuss this with people, I always have a very hard time making them understand the gravity of this situation. At first, the mind simply cannot take it in. And also, it sounds like ancient history to most people. After all the breed has survived another fifty years, hasn´t it? Aren´t our dogs great because of this concentration of greatness?
Let´s look at the facts: Blank to Ossi was a second-generation line breeding, one of the first done on their ancestral stock. At least one of those offspring (Domossi) died of a “heart-attack.” Domossi´s son Emperor, the product of another generation of line breeding, also died of a “heart-attack” (From Illena and the Seven Sires by Peggy Adamson). Alcor, the third of the “seven sires” to die of a heart attack, was related maternally. Jessy´s critiques from Germany clearly state that her temperament was not good, and people who knew Pericles of Westphalia have stated that he could not be shown because he was so fearful. Gretl v Kienlesberg (who was, incidentally, Jessy´s half sister) died of distemper along with most of her litter. Although distemper claimed the life of many dogs in those days, normally dogs´ immune systems are at an all time high while pregnant and lactating. One of Gretl´s famous grandget is said to have had no immune system at all.
Now over the past fifty years. But their tremendous genetic impact has a dark side, as well. We tend to beat ourselves up today -or worse, beat up each other -for the genetic frailty of our breed. But how can we defend ourselves against
something (things) that were instilled into them fifty or more years back? Our generation has inherited a gene pool that is too small. The worst problem we face is Cardiomyopathy and it is a defect that in most cases occurs after the dogs have reproduced. Line/Inbreeding has created vast improvements in type and structure, and has made our breed stand out among its peers as a pillar of consistency. But at the same time, it has so concentrated the “bad” genes that there may be no way out, particularly in the areas that relate to problems of the immune system, (e.g. thyroid disease, allergies, vaccine titres, autoimmune syndromes) and our heart-related diseases. Cardiomyopathy, arguably, could and should be relegated to the classification of diseases of old age, from which there is no escape. However, we see this scourge affecting even our young dogs.
No breed of animal is ruined in great leaps, but in tiny increments. Every time a breeder makes a bad or self-serving decision, a tiny step is taken towards the end of the breed. We can´t even see these steps most of the time because the course of breed history changes rapidly. A dog that is used sparingly in his lifetime may produce one over bred son and a dog that is used too much may find very little of his contribution around ten years later. A breeder sometimes justifies introducing genetic garbage into their line with the old saw, “I´ll
breed that out later.” One thing you can be sure of about breeding is that the second you breed flawed individuals you breed those characteristics IN. Only spaying and neutering ever “breeds” traits out! This is the one similarity I can think of between computers and genetics – GIGO – or (for those of us not computer literate) “Garbage In … Garbage Out.”
I don´t really want to bring out this information without a solution being offered – but I´m not sure there is one. People have suggested using only older dogs for breeding, but I´m not sure that is enough. Honesty between breeders would be a vast help, but since we typically attack the very people who try to be the most honest, you can´t really blame them for “going underground” the next time. What is needed is a general awareness that the Doberman breed is not here to serve anyone´s personal aggrandizement, but that we are here to serve the breed. We need to begin to make even the tiniest decisions with the breed´s future in mind and not our kennel name, the next show season or the next National. We need to give our pride away and live to serve the breed. We need to talk, to really communicate about the dogs, to make informed decisions. And we need to own our mistakes with the same grace we bring to our successes.
PART 2:: REVISITED:
by Margi Bragg, ADPEF Historian www.adpef.org
Reprinted with permission obtained by Marj Brooks
Or Never Let Fear Drive Your Bus
When the above article appeared in the summer 1999 D.Q., a mere ten years ago, I had no idea it would prove to be prophetic. I did know that the breed had some problems, serious problems, which were affecting health, longevity and worst, people´s perceptions of Doberman ownership. I did know that we also had some societal problems. Insurance companies didn´t want to insure us; PETA was loud, obnoxious and dangerous, urban communities needed to solve their dog problems. All of this taken together meant that the glory days of a large cropped and docked breed were over. What I didn´t foresee was that 1) the fancy would grow old and not replace itself. 2) The economy would tank and 3) that the Animal Rights Loonies without ever scoring a real victory against us would insidiously change our perception, “raise our conscience.” What I didn´t foresee was that guilt would so become a part of our approach to breeding that we would spay and neuter ourselves nearly to extinction. You may be wondering why I´m cramming all of the topics above into one article. I want you to understand he “Big Picture.” All of the above is one thing-one war, we are being attacked on many fronts, but it is one war. It is about a paradigm shift in America, a paradigm shift in which our rural and agricultural history is becoming increasingly urbanized. Urban mentalities have no connection with the realities of producing animals. Urban mentality is disconnected from the nature of life. It is disconnected from the inevitability of death. Those of us who insist on creating lives, in our case Dobermans, are being made to feel guilty and sadly, it is this guilt more than anything else that is now destroying the fancy and our breed.
The only thing I can guarantee when I produce a puppy is that it will die. When, where and how is beyond my capacity as a breeder. We are being held to a higher standard than human parents and that is ridiculous. Puppy buyers come wanting a guarantee of unlimited life. They believe they can purchase insurance against pain by buying a well-bred dog. They can dabble in something alive without experiencing the pain that comes with it. This is disconnected, urban thinking. We breeders have absorbed this thinking and are trying valiantly to produce a dog that is devoid of all medical problems. In the course of that pursuit, we are spaying and neutering everything less than 100 %. What you need to know is that by the time science gives us the tools we need to do that, there won´t be anything left to breed from. We will have been guilt-driven to extinction or at least will have created another genetic bottleneck. Genetic disorders are not causing the demise of purebred animals, but guilt is.
We have to do a number of things this instant if we are to be proper guardians of this Breed.
1. We have to identify and change our guilt-driven and fear-driven actions. Remember our Doberman temperament.
2. We have to fly in the face of AR´s and legislators who are pushing guilt. We must not absorb that guilt.
3. We have to begin to culture young people to take over for us.
4. We have to bear in mind the big picture and resist America´s paradigm-shift.
5. We have to breed dogs, lots of dogs.
6. We have to be publicly proud of our dogs and restore the cache´ and glamour of the show dog.
7. We have to behave with decorum and sportsmanship so that people will be drawn to our sport, not repelled by it.
8. We have to quit blaming and shaming anyone who breeds a dog that dies, including ourselves.
We have all forgotten to take a lesson from the Dobermans we so admire -watchful, fearless, alert, loyal, brave. We have become so tired, so poor, so guilty, so consciousness-raised and so spineless that we are letting the breed slip through our fingers. Entries at dog shows are pitiful, the amount of anti-dog legislation is pitiful, registration numbers are pitiful, letting a few crazy people tell us we shouldn´t crop and dock is the most pitiful. Where is, what has become of OUR temperament? The time has come as in the movie Network to stand up and say “I´m mad as hell, and I´m not going to take it anymore.”
Breeder/Exhibitor Ed, Health
submitted by Mary Korevaar, Glengate Reg’d
Dobermans appear to be more susceptible to the hypersensitivity reactions that can be caused by sulfa drugs. It is probably best to avoid using the following drugs in Dobermans, if possible.
Sulfa drugs:
Tribrissen (Trimethoprim/Sulfadiazine)
Ditrim (Trimethoprim/Sulfadiazine)
Bactrim (Trimethoprim/Sulfadiazine)
Septra (same as Bactrim)
Cotrim (same as Bactrim)
Comoxol (same as Bactrim)
Albon (Sulfadimethoxine)
Bactrovet (same as Albon)
Primor (Sulfadimethoxine/Ormetoprim)
Azulfidine (Sulfasalazine)
Apo-Sulfatrim
Novo-Trimel
Dobermans may develop an immune complex polyarthropathy and occular sensitivity to these drugs. However, not all Dobermans will react adversely to the above drugs so the use of these drugs may be worthwhile if the benefits of treatment outweigh the risks of an adverse reaction. That is for you and your veterinarian to decide.
Breeder/Exhibitor Ed, Breeding/Genetics
As you can see, the descriptions in the standard are all based on “correct” proportions. For example, when you see a dog that has ski slope topline, you know that it is incorrect even if the back is a straight line from the wither to the slightly rounded croup. The straight line is based on correct proportions, not the incorrect proportions that may be on the dog you are observing. If the shoulder is very straight and the back is a straight line from the highest point, which may be not be the wither, then that line will be greatly exaggerated into the dramatically sloping line. If the rear is over-angulated in relation to the front, the rear may be lower causing a sloping topline, The standard is very exact and has a reason for every explanation. Why is fill and underjaw so important? The standard explains why. Is there anything the standard doesn’t address? Pigment is not mentioned anywhere. Other than that, if you wonder about something, go to the section of the standard that addresses it. The standard is a great reference. It clearly states what should be there. If you can’t find what you’re looking for in the section that describes it, then it’s a deviation, even if it’s something you really love! As Doberman judges it’s our responsibility to preserve the breed as it was meant to be, which is through application of the standard. Personal preference can fall within the standard and there is room for it in many sections. Some sections are so specific that we must learn to like what is correct. As breeders, exhibitors, and judges, we are responsible for preserving this great breed as it was meant to be – as our standard so specifically directs us.
(Test your eye for proportion below)
Check yourself
Which dog has the correct proportions, A, B, or C?
Answer
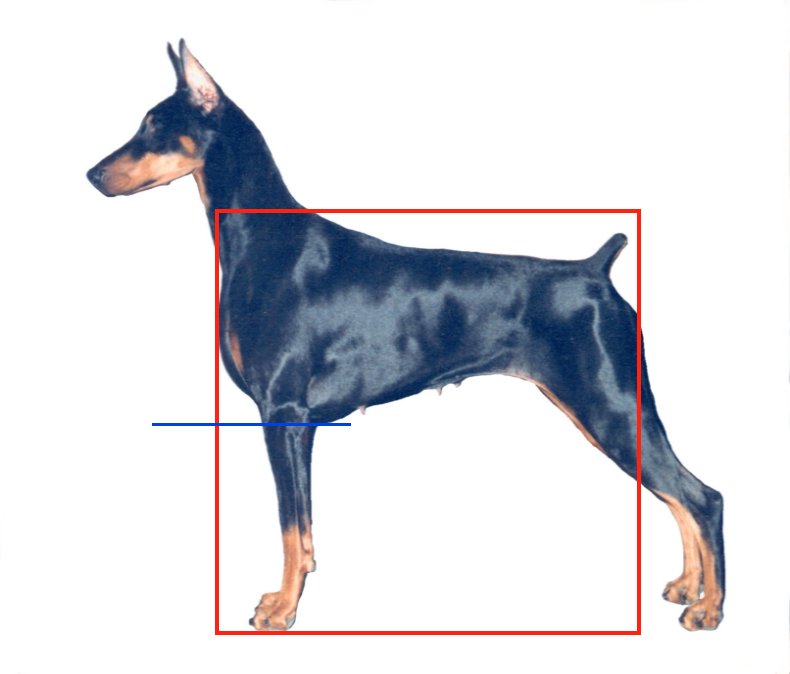
Dog “B” is correct
Dogs A & B measure square, while dog C measures too short horizontally. Dogs A & C have more length of leg than depth of body. Dog “B” has the correct proportion of body depth to length of leg as well as measuring square.
Click the following links to read more articles in the “Dobermans in Detail” series:
Size, proportion &substance
Head
Neck Topline and Body
Forequarters
Hindquarters
Coat
Gait
Temperament
Conclusion: test yourself
- by Linka Krukar submitted by Marj Brooks
Breeder/Exhibitor Ed, Breeding/Genetics
Energetic, watchful, determined, alert, fearless, loyal and obedient. The judge shall dismiss from the ring any shy or vicious Doberman.
Shyness: A dog shall be judged fundamentally shy if, refusing to stand for examination, it shrinks away from the judge; if it fears an approach from the rear; if it shies at sudden and unusual noises to a marked degree.
Viciousness: A dog that attacks or attempts to attack either the judge or its handler, is definitely vicious. An aggressive or belligerent attitude towards other dogs shall not be deemed viciousness.
The assessment of temperament begins with “reading” the dog’s eyes. The dog should be interested, confident, and curious. The dog should feel good about himself. When the Doberman stands on its own and when it moves you will see temperament. A dog that acts like a robot or stares blindly at a piece of bait is not displaying true Doberman temperament. Dogs are “only human” and do make mistakes, have feelings and emotions. They may feel like “showing/ working/performing” one day and not another, just like the rest of us. In the ring, the Doberman should be allowed to show his personality, respond, react, and just be a Doberman. We have a proud breed and require a very versatile temperament.
The judge shall dismiss from the ring any shy or vicious Doberman – the dog should be mentally sound and stable. Neither of these should be tolerated. This dog is too powerful to reward for poor temperament – if it’s not tolerated in the ring, the dogs won’t be bred and carry this on to future generations.
Shyness – A dog that moves while being examined should not be faulted if he recovers and can be examined with no trouble. This is a breed that should react to things and behavior that may initially seem shy, could be that of surprise. The dog should be socialized before attending shows. If the dog can’t be examined without the assistance of the handler, he should not be in the ring – no matter what the age. Even a dog with a very stable temperament can have a bad day. Do NOT ever tolerate a shy dog under any conditions!
Viciousness – This is a breed where most males are not tolerant of other males (bitches can be this way too). Dogs may try to make eye contact with other dogs, and “talk” to each other. This is NOT viciousness, it is a Doberman. If on the other hand, the dog acts threatening to a person or can’t be controlled, he will be disqualified from the ring. If the dog is not under control, he will be excused or disqualified accordingly.
Click the following links to read more articles in the “Dobermans in Detail” series:
Size, proportion &substance
Head
Neck Topline and Body
Forequarters
Hindquarters
Coat
Gait
Temperament
Conclusion: test yourself
by Linka Krukar submitted by Marj Brooks



